COVID-19 Took Black Lives First. It Didn't Have To.
Category: News & Politics
Via: kdmichigan • 5 years ago • 3 commentsBy: Duaa Eldeib, Adriana Gallardo, Akilah Johnson (MSN)

Larry Arnold lived less than a mile from a hospital but, stepping out of his South Side apartment with a 103-degree fever, he told the Uber driver to take him to another 30 minutes away.
Charles Miles' breathing was so labored when a friend called to check on him that the friend called an ambulance. Still, Miles, a retired respiratory therapist, was reluctant to leave his home.
Close family support had helped Rosa Lynn Franklin recover from a stroke several years ago, but when she was admitted to the hospital in late March, her daughter could do little more than pat her on the back and say goodbye.
All three were among the first people to die of COVID-19 in Chicago, and all three were African American. Their deaths reflect the stunning racial disparity in the initial toll of the virus. Of the city's first 100 recorded victims, 70 were black.
As the pandemic has spread, that gap has narrowed, and Latinos now make up the largest portion of any reported demographic of confirmed cases across Illinois, state data shows. But the disparity in black deaths persists. As of early May, African Americans, who make up just 30% of Chicago's population, are about half of its more than 1,000 coronavirus deaths.
It has been well established that African Americans are dying of COVID-19 at a disproportionate rate in cities across America. ProPublica sought to explore the problem by examining the first 100 recorded deaths in Chicago, a city with a rich and often troubled history on issues of race.
Using a database obtained from the Cook County Medical Examiner's Office that listed the names, health and location information of all COVID-19-related deaths, reporters reached out to the families and friends of each person who died. Reporters ultimately spoke with those who knew 22 of the victims; gleaned details about the lives of many others from obituaries and social media posts; and interviewed experts, medical professionals and government officials to understand how and why those first 100 died.
The racial disparities in coronavirus deaths have largely been attributed to endemic and entrenched inequalities in Chicago — decades of disinvestment in the predominantly black neighborhoods on the South and West sides that have left residents with fewer jobs, poorer health and diminished opportunities. Those forces often are portrayed as intractable and, during a pandemic, nearly impossible to fix.
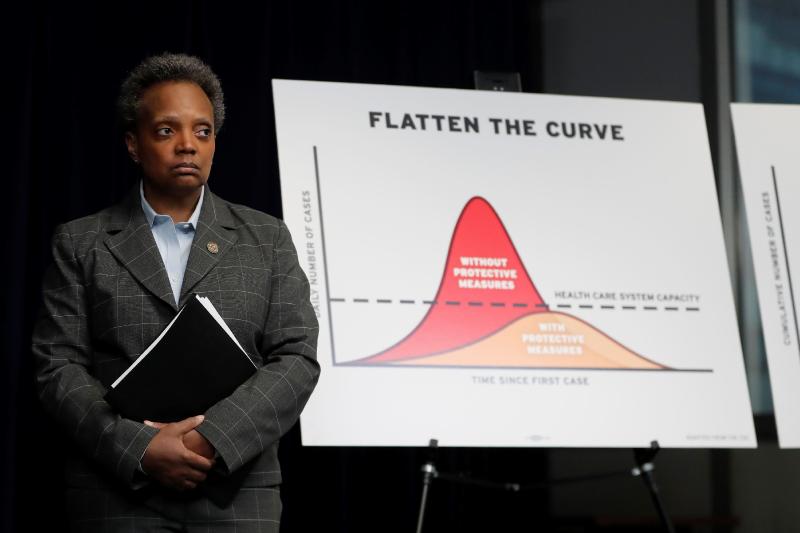
Chicago Mayor Lori Lightfoot acknowledged the challenge when she spoke publicly about the disparities last month and announced a plan to address them.
"We're not going to reverse this in a moment, overnight, but we have to say it for what it is and move forward decisively as a city, and that's what we will do," she said. "This is about health care accessibility, life expectancy, joblessness and hunger."
While all this is true, ProPublica's reporting also revealed other patterns, factors that could — and should — have been addressed and which almost certainly exist in other communities experiencing similar disparities. Even though many of these victims had medical conditions that made them particularly susceptible to the virus, they didn't always get clear or appropriate guidance about seeking treatment. They lived near hospitals that they didn't trust and that weren't adequately prepared to treat COVID-19 cases. And perhaps most poignantly, the social connections that gave their lives richness and meaning — and that played a vital role in helping them to navigate this segregated city that can at times feel hostile to black residents — made them more likely to be exposed to the virus before its deadly power became apparent.
Many of the first 100 recorded Chicago COVID-19 victims led lives threaded through with community and civic involvement, powerfully connected to their city, to friends and family. Some had led careers of service, like Patricia Frieson, a retired nurse, and Rhoda Hatch, a former teacher, and Carl Redd, a U.S. Army veteran. Their small businesses helped shape their corners of the city; Hardwell Smith, 85, arrived in Chicago as part of the Great Migration from the Jim Crow South and established gas stations and auto repair shops on the South Side. They were church deacons and musicians; doting uncles like 32-year-old Carl White and nurturing mothers like Juliet Davis, who, despite her limited means, fed the homeless who lived under a neighborhood viaduct.
Most of the first 100 lived in majority-black neighborhoods, according to an analysis of medical examiner data; hardest hit were South Shore, Auburn Gresham and Austin, where the median income for 40% or more of the residents in each community is less than $25,000.
Many were already sick, with underlying health conditions. Seventy-eight of them had hypertension and 53 had diabetes. Just 12 had one health condition, and only five people had no comorbidities. James Brooks, a 27-year-old black man, was the youngest to die.
"I'm not surprised because every natural disaster will peel back the day-to-day covers over society and reveal the social fault lines that decide in some ways who gets to live and who gets to die," said Dr. David Ansell, senior vice president for community health equity at Rush University Medical Center. "And in the United States, those vulnerabilities are often at the intersection of race and health."
Ansell, who wrote "The Death Gap: How Inequality Kills," has spent decades documenting the life expectancy gap between black and white Chicagoans, which is the largest in the country. Structural racism, concentrated poverty, economic exploitation and chronic stress cause what's known as biological weathering, Ansell said, where the body ages prematurely and results in earlier death.
Who dies first is different for each pandemic, said Dr. Howard Markel, director of the Center for the History of Medicine at the University of Michigan. The coronavirus's earliest victims, he said, were the most vulnerable.
"They're not quite forgotten, but we don't pay close enough attention to the health and well-being of this segment of the population," he said. "Then a microscopic organism comes and topples them over."
They were vulnerable, but their deaths cannot be dismissed as inevitable.
Phillip Thomas, 48, started to feel sick while working a day shift at the Walmart in Evergreen Park. A diabetic, he was cautious about his health, and he reached out to a doctor, who told him to stay home and self-quarantine in case he had the coronavirus.
About a week into his bedrest, Thomas told his sister Angela McMiller that he was having a hard time standing up and was vomiting, no longer able to keep anything down. She encouraged him to go to the emergency room, but he didn't immediately go, citing the doctor's advice to stay home.
Within a couple of days, he called an ambulance, which took him to Jackson Park Hospital, where he was intubated. Two days later, on March 29, he died, in the hospital where he was born.
When McMiller next saw her brother, it was at his funeral, which only 10 people could attend because of social distancing requirements. "It was devastating," said McMiller. "My mother fell down, my brothers cried."
McMiller is upset that her brother was told to stay home when he was sick, particularly considering the additional risks posed by his health history.
"It shocked me," she said. "He was diabetic."
Since the earliest days of the pandemic, the Centers for Disease Control and Prevention's guidelines have emphasized staying home when symptoms are mild. "Most people with COVID-19 have mild illness and can recover at home without medical care," the CDC says on its website. It recommends people call a doctor before going to get care in person, unless experiencing emergency signs like trouble breathing, blue lips or chest pain.
But experts told ProPublica that this one-size-fits-all advice does not account for the fact that African Americans are not only more likely to have preexisting conditions that increase their chances of bad outcomes, but also have a long-standing wariness of the health care system.
"There is this distrust between black communities and health care systems based on this fraught history of how health care systems have exploited and abused black people," said Dr. Uche Blackstock, an emergency medicine physician in Brooklyn and the founder and CEO of Advancing Health Equity. "What happens as a result of that is that patients don't want to interface with the health care system."
In addition, doctors said patients may delay seeking care out of a fear of the medical bills, lack of insurance or transportation barriers — all of which underscores the need for targeted guidance. So instead of encouraging staying at home, these doctors want guidance to encourage African American patients to proactively seek care before symptoms get out of hand.
Dr. Mira Iliescu-Levine, a pulmonary critical care doctor at The Loretto Hospital on Chicago's West Side, is concerned that African American and Latino patients are waiting to come to the hospital after their symptoms become too severe.
"You end up with an overwhelming clinical picture, almost like a tornado, that's very hard to stop," she said.
She said she wants patients, especially her African American patients with diabetes, obesity and other comorbidities, to seek care when they have "innocent symptoms" like a cough, runny nose, itchy eyes or low-grade fever.
Earlier treatment does not guarantee a better outcome, she said, but it can give the patient a fighting chance.
"Reach out," she said. "Don't wait."
Asked whether the CDC would consider tailoring its recommendations to reflect the underlying health conditions and barriers to care in African American communities, a spokesperson said the "CDC is collecting data to monitor and track disparities among racial and ethnic groups … to help inform decisions on how to effectively address observed disparities. … We will continue to update our recommendations as we learn more."
The CDC spokesperson said the agency has increased "engagement with organizations and other partners representing and serving racial and ethnic minority groups to identify gaps in the current response efforts," and that people should "never avoid emergency rooms or wait to see a doctor if you feel your symptoms are serious."
On the first day, Willie Flake, a 72-year-old mechanic, lost his ability to taste. Then, he lost his appetite. With each new coronavirus symptom he experienced, his sister Betty and her daughter Yolanda pushed him to go to the hospital.
But Flake, who had diabetes, stayed home because he thought his symptoms were not severe enough to go to the emergency room. He soon developed a fever. By the fourth day, he had trouble breathing.
Flake took an ambulance to Rush University Medical Center on March 27, where his condition appeared to stabilize before worsening again.
"They say, 'Don't come in until your fever is high and you can't breathe,'" Yolanda Flake said. "That's the part where I feel like they failed him. He waited until he couldn't breathe and it was too late."
In the early hours of April 1, his sister and niece put on masks and gloves and looked through the glass window of his hospital room. He had been like a father to Yolanda, attended every graduation, from kindergarten through college, and had recently accompanied her to buy a car for her daughter, his 23-year-old grandniece, LaSeanda.
Yolanda said she wished she could have been with him inside the room, regardless of the risks.
"I wanted to touch him," she said. "I wanted to talk to him before he took his last breath. I couldn't say it through the glass door."
And then, his heart stopped.
"He waited at home," Yolanda said, "and he was dying already."
Struggling Hospitals
Larry Arnold also waited, not because he was instructed to, but because he didn't trust his neighborhood hospitals.
Two — Jackson Park Hospital and South Shore Hospital — sit within five minutes of his home. Both are century-old nonprofit facilities that serve majority low-income and uninsured patients on the South Side. When Arnold started to feel sick in mid-March, he worried that if he called an ambulance, it would take him to one or the other. He didn't want to go to either.
"What upsets me is that we don't have adequate medical facilities where we can go to and feel like we'll be cared for," his niece Angelyn Vanderbilt said. "I'm sure they're very good people … but the consensus in the community is that those hospitals are inadequate and they have been for years."
After his fever didn't subside for a few days, Arnold, who was 70 and had chronic obstructive pulmonary disease, or COPD, knew he couldn't wait any longer, his family said. He got into an Uber with a temperature of 103 and told the driver to take him to Advocate Christ Medical Center in Oak Lawn, some 30 minutes away.
On March 31, 16 days after he was admitted, the nurse put the phone to Arnold's ear one last time.
"We told him to be strong and to continue to fight," Vanderbilt said.
He died about an hour later.
People who live on Chicago's South and West sides are often at a geographic disadvantage during medical crises because the hospitals that are closest to them frequently are those with fewer resources.
Illinois Gov. J.B. Pritzker acknowledged the hardships at a press briefing last month. "The safety-net hospitals are challenged in our state, and the availability of health care in communities of color has been at a lower quality or lower availability than in other communities," he said.
The city's safety-net hospitals, facilities that serve a large portion of low-income and uninsured patients regardless of their ability to pay, don't have the private-insurance patient base or the cash reserves to fall back on during a pandemic that many larger hospitals have, said Larry Singer, associate professor at the Beazley Institute for Health Law and Policy at Loyola University Chicago School of Law. Some are millions of dollars in the red and housed in aging buildings. And while their mission is a valiant one, he said, they have not been able to respond to the coronavirus as quickly or with the same equipment and staffing.
"They're trying to fight the same fight as everybody else with one arm tied behind their back," Singer said. "They deserve the resources to do an even better job. I'm truly impressed by what they are trying to achieve during a time of crisis."
Tim Caveney, president and CEO of South Shore Hospital, said that limited resources is one reason safety-net hospitals have struggled to earn the trust of the communities they serve. "Safety net [hospitals] have gotten a bad beat because we don't have much money. It's a funding issue," he said, adding that the pandemic has aggravated South Shore's financial issues. Not only have lucrative elective surgeries been postponed, but COVID-19 patients often require complex and lengthy care, which can be expensive.
Dr. Khalilah Gates, an African American pulmonary and critical care specialist at Northwestern Memorial Hospital who has family on the South Side, said she is painfully aware that some black patients may prefer to "wait it out" or travel to distant hospitals.
"Both of those are very common phenomenons," she said. "Not all community hospitals, but many of the community hospitals in those communities lack the resources that offer security to the residents in those areas."
ProPublica spoke with several families who said their loved ones either delayed care because they didn't want to go to neighborhood hospitals or ultimately wound up in those hospitals as a last resort.
Miles, the retired respiratory therapist, had worked for about 40 years at Northwestern Memorial Hospital providing breathing treatments for patients there. When he started feeling sick in mid-March, he knew what resources he might need.
A friend called him on March 22 and heard his labored breathing. He told Miles that he was calling an ambulance, but Miles resisted, in part, because he didn't want to be taken to Jackson Park, the nearest hospital.
"He should've been in there a week before that," said his sister Roselle Jones. "But he was insistent on not going."
The paramedics said that they had to take him to Jackson Park because it was the closest hospital. Miles' family asked that he be transferred to another hospital, but once he tested positive for the coronavirus, a doctor told the family that Miles couldn't be moved, Jones said.
By the end of the week, Miles had been sedated and placed on a ventilator. He died on April 3.
"We wanted him out of there. We wanted him somewhere he could get some good care," Jones said. "The doors should be closed, and the building torn down."
Philman Williams' family also said they tried in vain to get him transferred out of Jackson Park after an ambulance took him there. Williams, 70, worked as a doorman at a luxury high-rise where residents dubbed him the "Mayor of Michigan Avenue" for his charm and good humor. Not only was his doctor at another hospital, but the family worried about the quality of care he would receive.
A day after he was admitted, their concerns were amplified by a news story detailing reports from employees that the hospital did not have enough personal protective equipment, prompting nurses to avoid entering patient rooms.
Nurses who were sick and those afraid to come to work because they had elderly relatives at home have led to staffing shortages, said Kindra Perkins, a representative with National Nurses United, the union that represents nurses at Jackson Park. One day, an ambulance couldn't drop off a patient because there were only two nurses working in the emergency room, she said.
"The nurses deserve to have the resources that they need to provide the quality care in that community, and the people in that community are just as important as the folks on the North Side of Chicago," Perkins said.
Margo Brooks-Pugh, a vice president of development at Jackson Park Hospital, did not answer specific questions, but she wrote in an email that the hospital takes patient and staff safety seriously.
"Jackson Park Hospital follows all guidelines and standards as related to patient care and safety," she wrote.
Austin, on the West Side, is one of the city's largest and most chronically underserved areas. It has become a hot spot for COVID-19 cases. The Loretto Hospital, a small nonprofit that has been an anchor in the community for more than 90 years, is the primary provider in the area. Like many of the safety-net hospitals in Chicago, it has struggled financially for years.
When Asberry Stoudemire Jr., a 54-year-old diabetic, got a runny nose, then felt his blood sugar levels begin to fall, his family knew he needed to get care quickly. He also had a history of congestive heart failure, which had forced the avid stepper and musician to retire early from his job as a certified nursing assistant. The Loretto Hospital wasn't their first choice — or their second. But it was the closest. Within hours of arriving at Loretto, his condition deteriorated so rapidly that he was sedated and intubated.
His daughter Miranda Stoudemire said she had trouble getting a clear sense of what was going on in the 10 days her father spent in the hospital's recently reopened 15-bed ICU. Loretto couldn't afford to keep the unit up and running before the pandemic, a fate hospital administrators said they fear could be repeated without an infusion of cash as the pandemic continues.
"He was saying, 'I know one thing, I'm not going to Loretto,'" she said. But he did, and she is resolute in her belief that her father would have lived longer had he been at a better resourced hospital. His family tried having him transferred but said they were told he was too critical to be moved.
"I feel like he didn't even have a chance to fight," she said.
He died March 29.
Mark A. Walker, spokesman for The Loretto Hospital, said that the hospital has the capacity to care for its patients and is doing its best to communicate with families.
"This hospital has gone through hard times," he said. "We're doing everything we can. We're learning along with everybody else. But better resourced communities don't have to fight for the same divvy of health care resources that we do."
Although L.B. Perry was 78 and suffered from hypertension and diabetes, nothing usually kept him in bed. So when he didn't wake at 6:30 for his morning oatmeal and coffee, his family began to worry.
As he grew weaker and needed help walking to the bathroom, his family urged him to go to the hospital. After a few days, he relented and went to Holy Cross Hospital in Chicago Lawn on the South Side, but he was sent home, his daughter Vernice Perry said.
"That's why I'm so upset," she said. "He was in the age bracket, and he has all these health conditions, and he had some of the symptoms."
His condition worsened at home, and his daughter said she begged him to let her drive him to another hospital. Four days later, his wife called an ambulance in the early morning of March 30, and he returned to Holy Cross Hospital. He died on April 2.
Dan Regan, a spokesperson for Sinai Health System, did not answer questions about specific patients, citing privacy restrictions. He said that its hospitals, including Holy Cross, are "thoroughly prepared for handling the COVID-19 pandemic," having created dedicated COVID-19 teams, using mobile triage trailers outside facilities to handle sick patients, and isolating COVID-19 patients in specialized rooms.
"It is worth noting though that the challenging nature of COVID-19 is that patients can look fine at one point and be discharged home with monitoring and follow-up, only to deteriorate and have to return to the hospital," said Regan. "This has been seen in many cases nationwide."
At least 110 patients from community hospitals, including Holy Cross, have been transferred to Rush University Medical Center, a large, well-equipped facility that has been touted as having been "built for a pandemic."
"They're really patients that otherwise, in all likelihood, would not survive at those hospitals," said Dr. Paul Casey, Rush's acting chief medical officer. "The resources just aren't the same. Nor is the ability within critical care to provide a lot of the life-saving therapies."
The City's Response
On April 6, when Mayor Lightfoot publicly announced that the coronavirus was disproportionately affecting the city's black residents, the virus had been in Chicago at least since January, and more than 100 people were dead. The majority were black.
"When we talk about equity and inclusion, they're not just nice notions," Lightfoot said at the time. "They are an imperative that we must embrace as a city. And we see this even more urgently when we look at these numbers and this disparity. It's unacceptable. No one should think that this is OK."
That day, the city announced the Racial Equity Rapid Response Team in partnership with West Side United, with a goal to "bring a hyper local public health strategy to targeted communities." In the weeks since, the team has held tele-town halls, delivered thousands of door hangers and postcards with targeted information, and distributed 60,000 masks for residents in the predominantly black communities of Austin, Auburn Gresham and South Shore.
Dr. Allison Arwady, the city's public health commissioner said in an interview that officials had worked behind the scenes to combat rumors that black people couldn't contract the coronavirus, reaching out to community and faith leaders on the South and West sides in February and March to let them know the city was seeing cases across all races.
Arwady said the department at first hoped to contain the spread. It had tracked the cases for weeks as the virus crept through the city, and then exploded. By the end of March, more than 40 Chicagoans had died from the virus, according to the county medical examiner data, though the city said its tally of deaths was less than half of that.
For the most part, Lightfoot has received plaudits for her handling of the pandemic. Illinois was one of the first states in the country to release statistics on COVID-19 deaths by race. Lightfoot herself has even become something of a national political star, with viral videos and memes of her urging residents to stay home. She also gave several high-profile interviews discussing the disproportionate impact of COVID-19 on black communities and emphasizing the importance of tracking demographic data.
The city also encountered some challenges. Early on, it found that up to 30% of the testing data it collected didn't list race. At the April 6 press conference, which came one day after a WBEZ news report detailed the death disparities, the city released a detailed race analysis. The city also issued a public health order mandating demographic data of COVID-19 cases be reported in hopes of being better able to track and assist individuals and communities falling victim to the coronavirus.
Still, to some in the community, the city appeared a step behind. Niketa Brar, co-founder and executive director at Chicago United for Equity, which advocates for racial equity in the city, said officials didn't do enough to engage the communities they knew would be hardest hit. As soon as the virus entered Chicago, she said, the city should have used racial, health and economic data to predict where it would take hold and then begin working with residents in those communities on how best to protect and support them. The Racial Equity Rapid Response Team was dispatched much later, she said.
"We've seen enough maps to know what the next map is going to look like," Brar said. "And yet we consistently fail to engage those who are closest to the harm time and time again."
Lightfoot said in an interview Friday she believes the city responded robustly to the virus from the start.
"I feel pretty good about where we are," she said. "Has it been perfect? Has any of this been perfect? No, because you're not going to be able to undo literally 100-plus years of racial disparities across black and brown Chicago. But I'm going to be a champion for people in my city, and particularly people who look like me and who grew up in circumstances like mine."
The Perils of Connection
It made sense that they were out on Election Day — Revall Burke, a 60-year-old city worker, who served as an election judge for the March 17 primary, and John J. Hill Jr., 53, who was campaigning for a friend outside of City Hall, handing out masks and shaking hands.
Their community connections had shaped their lives. Both grew up in public housing. Burke went on to help form a building committee to give back to the neighborhood, including organizing picnics where he would give away school supplies. Hill, who built a successful business and counted among his proudest moments catering a campaign event for Barack Obama, met his wife at the iconic Rock 'N' Roll McDonald's where she worked as a teenager. He came in to buy ice cream nearly every day; when she was sick, he got her a "get well soon" card signed "the ice cream man," sparking a 40-year romance and two sons.
For black residents in a city as segregated as Chicago, connections to family, church and community can be a vital resource. During the 1995 Chicago heat wave, connectedness sometimes meant the difference between life and death: Sociologists found that compared with more affluent neighborhoods, Auburn Gresham had fewer deaths, in part because residents knew their neighbors and checked on one another during the extreme temperatures, just as they did every day.
Yet those deep connections put black Chicagoans in harm's way as the novel coronavirus spread largely undetected, said Jaime Slaughter-Acey, a social epidemiologist at the University of Minnesota who did her doctoral work in Chicago. "What we're seeing in the time of COVID is that this virus has taken this really important, health-promoting resource [of social connectivity] that we've created and used it against communities of color."
Both men died on April 1, two weeks after the election.
The Chicago Department of Public Health and the CDC mapped one cluster of 16 known or suspected infections — and three deaths — dramatically illustrating the path the virus tore through families and friends who attended an intimate dinner, a funeral, a birthday celebration or a church service. Jennifer Layden, the department's deputy commissioner, said the case study shows how insidious the virus could be in social settings — even a gathering of just three loved ones could be deadly.
Eboney Harrell was aware of the risk and barred all visitors from stopping by after her daughter SaDariah brought home her newborn baby. A single mother, Harrell was an anchor for SaDariah, rarely leaving her side after she learned her daughter became pregnant. Harrell went to the doctors' appointments and hosted a circus-themed baby shower with custom T-shirts; hers read "Grandma." After her grandson was born at the University of Chicago Medical Center on March 19, she took every opportunity to hold him.
Her friends believe she may have gotten the virus at the hospital.
When it came time for Harrell to be the patient, nobody was allowed to be by her side. She died on April 4, alone.
A bedside advocate is important for anyone in the medical system but especially the seriously ill. Sociologists say that, though critical, barring visitors during the pandemic to contain the virus may inadvertently magnify its deadly impact.
Human connections had fueled Rosa Lynn Franklin's recovery after she suffered a stroke several years ago. Though Franklin had to retire from her longtime career as a social worker in her native Alabama, she filled her days with family, friendships and prayer. She moved to Chicago last year to be near her only child, finding a new community in extended family and a church down the street.
As COVID-19 encroached, Franklin, 64, became homebound, worried about how the virus might affect her fragile health. Despite all her precautions, she got sick, and by March 24, she was having such difficulty breathing that her daughter took her to the emergency room at University of Illinois Hospital.
"Because of social distancing, you can't really do a lot of touching," her daughter Jimeria Williams said, "so I just kind of patted her on the back and said, 'I love you, I'll see you.'"
Franklin was intubated the day after she was admitted, and while Williams was able to talk with the doctors, she could not communicate with her mother, not even by phone. It was the opposite of what had happened after the stroke, when Williams was a constant presence at her mother's bedside.
"I couldn't be there to hold her hand. I know she knew that, even though she was unconscious," she said. "I think that had a metaphysical impact on her health."
In the early evening of April 3, the hospital was able to connect Williams with her mother through FaceTime. A few minutes after hearing her daughter's voice, Franklin died.
Tags
Who is online


72 visitors
How can this be, I mean Chicago has been A Democrat city for how many years? Racial disparities? Must be fake news.
They complain when investment leaves the neighborhood or is directed elsewhere. But if you invested in the neighborhood, opened up new business, and thus, raised property values, they would complain of gentrification. They would would whine that rising property values are either driving people out of their homes (somehow) or that an influx of more well-off people or different ethnicities were destroying the cultural distinctiveness of their neighborhood.
So, you're damned if you do and damned if you don't.
How many times have we seen stories from all over the country of blacks holding large house or block parties, pictures showing attendees not wearing masks and certainly not distancing, in mostly in large democratic held cities?
Maybe this would be one of the causes?
Nah...that would be racist.