How does health spending in the U.S. compare to other countries?

This chart collection takes a look at how spending on healthcare in the United States compares to other OECD countries that are similarly large and wealthy (based on GDP and GDP per capita). The analysis looks at 2016 health data from the OECD Health Statistics database. These charts are based on data from the OECD, allowing for international comparisons; however, some values from OECD are reported as provisional or estimated and may not exactly match U.S. data reported in the National Health Expenditure Accounts.
Relative to the size of its wealth , the U.S. spends a disproportionate amount on health care:
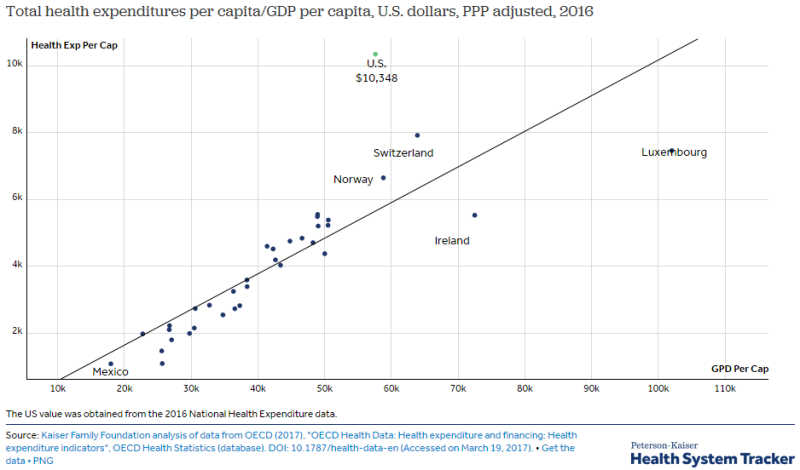
As would be expected, wealthy countries like the U.S., tend to spend more per person on health care and related expenses than lower income countries. However, even as a high income country, the U.S. spends more per person on health than comparable countries. Health spending per person in the U.S. was $10,348 in 2016 – 31% higher than Switzerland, the next highest per capita spender.
On average, other wealthy countries spend about half as much per person on health than the U.S. spends:
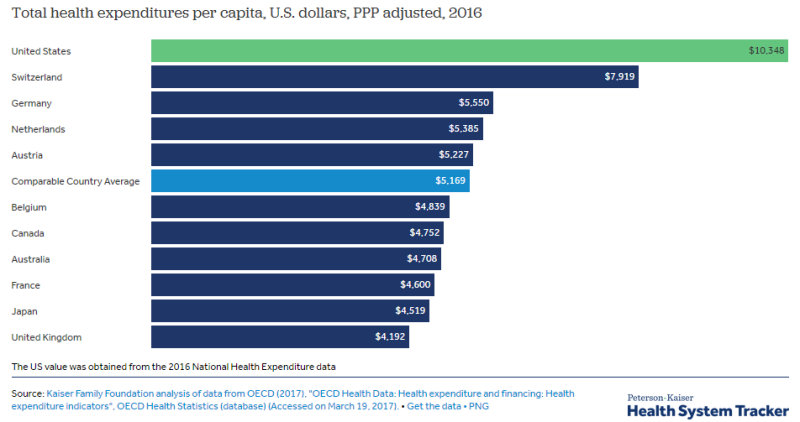
Because health spending is closely associated with a country’s wealth, the remaining charts compare the U.S. to similar OECD countries – those that have above median national incomes (as measured by GDP) and also have above median income per person. The average amount spent on health per person in comparable countries ($4,908) is just over half that of the U.S. ($10,348).
Since 1980, the gap has widened between U.S. health spending and that of other countries:
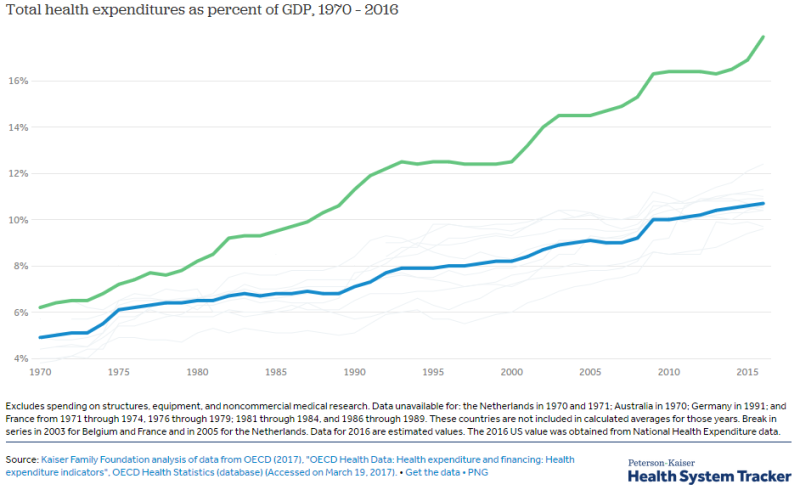
Over the past four decades, the difference between health spending as a share of the economy in the U.S. and comparable OECD countries has widened. In 1970 the U.S. spent about 6% of its GDP on health, similar to spending by several comparable countries (the average of comparably wealthy countries was 5% of GDP in 1970). The U.S. was relatively on pace with other countries until the 1980s, when its health spending grew at a significantly faster rate relative to its GDP. In 2016, the U.S. spent nearly 18% of its GDP on health, whereas the next highest comparable country (Switzerland) devoted less than 13% of its GDP to health.
U.S. health spending growth was higher during the 1980s, but has been similar since:
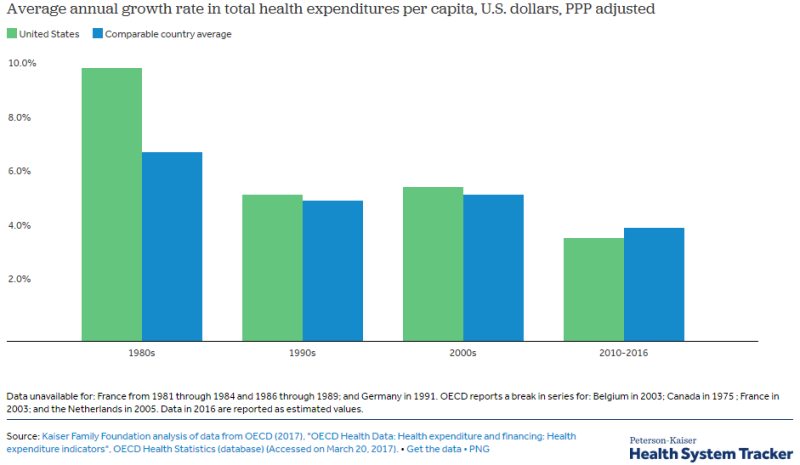
While the U.S. has long had higher than average spending, it has not always been such an outlier. The 1980s saw accelerated growth in health expenditures per capita in the U.S. The 10.1% average annual growth rate in the U.S. during the 1980s was the highest among comparable countries. The comparably wealthy countries saw an average of 7.0% annual growth during this period. Since 1990, health spending has grown similarly in the U.S. and comparable countries.
In recent years, health spending growth has slowed in the U.S. and in comparable countries:
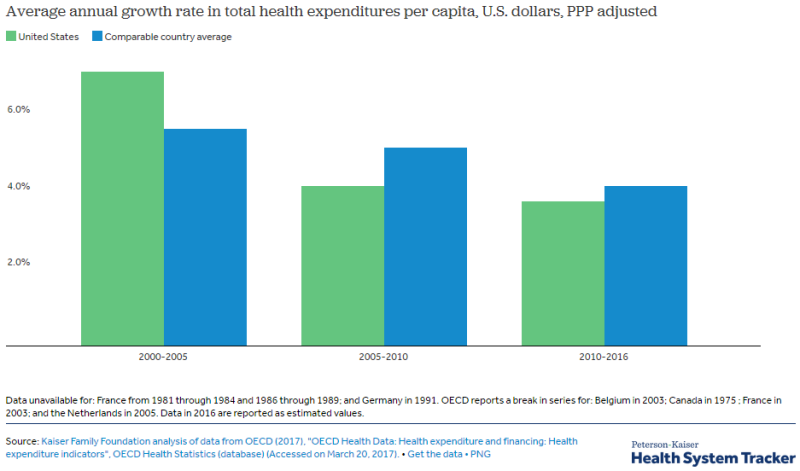
Health spending growth in both the U.S and comparable countries has slowed in recent years. In the 2005-2010 period, the U.S. saw a 4.2% average annual growth rate compared to 7.2% the previous five year period. Comparable countries also saw a drop to a 4.2% average annual growth rate during the 2010-2016 period, down from 5.2% on average in the 2005-2010 period.
While the U.S. has similar public spending, its private sector spending is triple that of comparable countries :
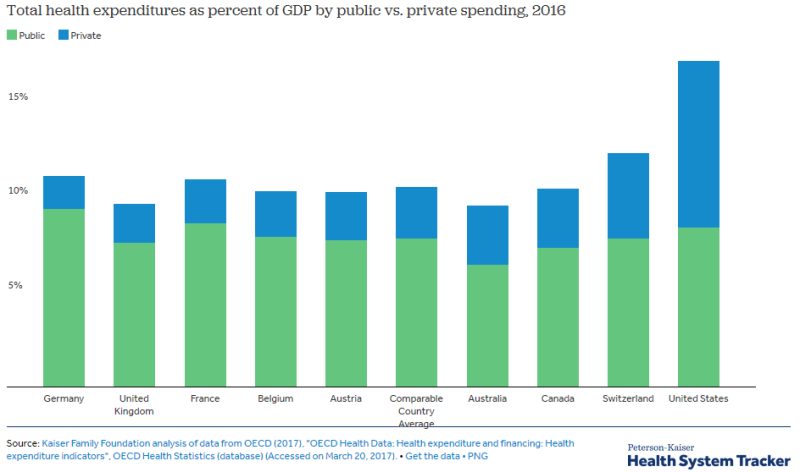
While the U.S. has much higher total spending as a share of its economy, its public expenditures alone are in line with other countries. In 2016, the US spent about 8.5% of its GDP on health out of public funds –essentially equivalent to the average of the other comparable countries. However, private spending in the U.S. is much higher than any comparable country; 8.8% of GDP in the U.S., compared to 2.7% on average for other nations.
The U.S. has increased both public and private sector spending at a faster rate than similar countries:
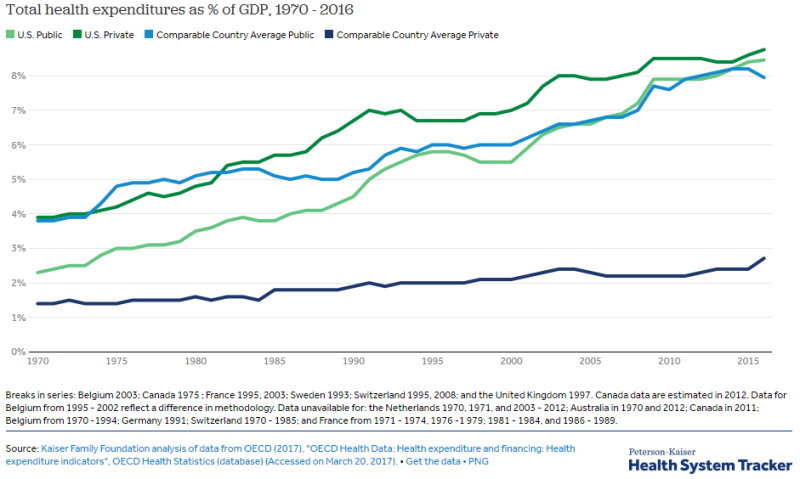
Over the last three decades, the U.S. has seen increased spending by both the public and private sectors. Comparable countries increased private sector spending from 1.4% to 2.7% of GDP from 1970 to 2016, while the U.S. increased private sector spending from 3.9% to 8.8% during the same period. In 2016, the U.S. spent 8.5% of GDP on health through public funds, a rate similar to comparable countries.
Tags
Who is online

47 visitors
Yesterday, I seeded an article about Bernie Sanders's "Medicare for all" plan . The conversation was lively... but amazingly empty, just as it was during the pre-Obamacare "debate".
Everyone has an opinion - often vehemently held - but nobody knows what they're talking about. It's kinda strange...
It's not as if the data isn't available. The site I'm seeding from today is excellent, and there are lots of others.
This isn't complicated: Americans spend a lot more on health-care than other developed nations... while getting shorter life expectancy in return. High cost, crappy results. Obviously unsatisfactory.
Europe has lots of different systems, spanning the spectrum from monolithic government (UK's NHS) to atomized private (Switzerland) and all of them give better results for less money than America's mess.
It might be a good idea to go see how others do it better, no???
Oh....the irony....
Yes. Our providers charge a lot more. Our providers make a lot more. Our lifestyles are appalling and we pay outrageous amounts for prescriptions.
But to the specific point.....nobody is saying our system could not be improved. What we're saying is that changing which company processes the claims is not actually an improvement.
So you're saying what should not be done.
Do you have anything to say about what should be done?
Actually....yes.
We have three issues to address. 1. Access to care 2. Cost of care 3. Lifestyle and general health
Issue 1: Access to care - insurance
The cost of insurance is driven by the cost of care, so we'll cover that in a minute. Keep the guaranteed issue and no pre-ex limitations of the ACA. They actually existed in small business plans for decades prior to the ACA in 38 states, so insurers know exactly how to manage them. Get rid of the individual mandate for good, as it is wholly unnecessary and hugely unpopular.
Then, do one of two things. Either make Medicaid a Federal-only program and bump the qualification level to 138% nationwide. ...or...and this is better... Make Medicaid a Federal-only voucher program and roll it into the healthcare exchange so those people can have the same coverage as everybody else. Then, combine the application for any other kind of US govt assistance with the application for Medicaid, and require any person receiving public assistance to demonstrate health coverage.
For those people who can afford insurance but just don't take it, make them responsible for their claims. Allow providers to submit unpaid bills more than 180 days old to the US Treasury for reimbursement. Then, have that bill deducted from that person's income tax refund until it's paid. When people realize they are going to be held responsible for their obligations, they will grow up and take care of their affairs.
Issue 2: Cost
Contrary to fantasy, you can't actually drive drastic cuts through the system and expect it to survive. Hospitals, providers, manufacturers and everybody else in that industry makes multi-year commitments based on projected revenue. You don't want them defaulting on their bonds and killing the teachers' and firefighters' pension plans.
However, you can slow and eventually halt the madness. Simply freeze Medicare reimbursement rates. Announce it a couple of years in advance, so everybody has time to plan. Set the drug price cap at some multiple of what other governments pay. For example, "Medicare will pay 10% more than the average cost of XXX drug in Canada, Australia, and the United Kingdom". Most private insurance plans drive their reimbursement rates as a multiple of Medicare payments, so slowing that train is key to everything.
When the federal govt stops "just paying more", it will stop enabling inefficiency. Systems will improve because the major stakeholders will feel a need to improve them. Currently, they don't. Under M4A, they certainly don't, and never will.
Further, we need to reintroduce medical questions for health insurance. The ACA unwittingly concentrates all the very sickest people into the very smallest pool. Prior to 2010, 38 states operated high-risk pools, where unhealthy individuals could get insurance, and then have very high their claims subsidized by all other insured people in their state. The ACA did away with those programs, and in doing so allowed insurers to get away from those high-risk individuals by simply declining to offer individual purchase plans. That's why the insurers who stayed have lost so much money and why so many have dropped out of that business along the way. The remedy for that is simple. Reintroduce those risk pools (or create a federal one), and force every health insurer to assume their proportional share of those liabilities. Now the sickest people can get the same insurance as the healthiest ones, and one small section of the population doesn't get bled to death.
Issue 3: Health
You can't have a serious discussion about outcomes without discussing obesity, smoking, poor diet, lack of exercise, and the hundreds of billions we spend because of the decisions some of us make. Obesity alone directly accounts for over 8% of total healthcare spending and smoking accounts for another 5%.
I believe it is the Constitutional right of every American to be fat and/or to smoke. But I'm not convinced it should cost the rest of us more money.
I know of no universal health-care system that does not carry a universal mandate.
If there is no mandate, and no pre-ex, then people would be foolish to take out health-insurance until they are sick.
The risk pool, having only sick people, would be impossible to manage.
Totally unnecessary, massively unpopular, and cataclysmic for the party that enacts it. Or did you think we came to a Donald Trump presidency because people like being forced to buy something.
We've dealt with this in employer-based insurance plans for decades with the use of an open enrollment window.
It is impossible to manage. Which is why the ACA has created such problems.
If you want to ignore the reality of ALL the successful systems in favor of what you imagine for the worst system in the developed world... go for it!